
The Future is in Focus: Nurturing Innovation and Collaboration in Pediatric Liver Transplantation
The WebApp is sponsored by: ![]()
Impact of Donor Age and Graft Type on Outcomes After Pediatric Liver Transplantation for Biliary Atresia
Ioannis Ziogas1, Dor Yoeli1, Megan A. Adams1, Katie R. Conover2, Amy G. Feldman2, Ronald J. Sokol2, Sarah A. Taylor2.
1Division of Transplant Surgery, Department of Surgery, University of Colorado Anschutz Medical Campus, Children's Hospital Colorado, Aurora, CO, United States; 2Department of Pediatrics, Section of Pediatric Gastroenterology, Hepatology & Nutrition, , University of Colorado Anschutz Medical Campus, Children's Hospital Colorado, Aurora, CO, United States
Introduction: We evaluated the effects of donor age and graft type on survival outcomes after liver transplantation (LT) for biliary atresia (BA).
Method: We performed a retrospective analysis of children with BA <18y who underwent first isolated LT using United Network for Organ Sharing data (02/27/2002-09/30/2025). Multivariable Cox regression included donor age group, graft type, recipient age group, laboratory MELD/PELD score, portal vein thrombosis (PVT), intensive care unit (ICU) status, and cold ischemia time (CIT).
Results: A total of 3,686 children with BA (<2y: 2,788 [75.6%] vs ≥2y: 898 [24.4%]) underwent LT. The donor age/graft groups were: <18y deceased donor whole graft (DDWG): 1,742 (47.3%), <18y deceased donor technical variant (DDTV): 791 (21.5%), 18-39y DDWG: 33 (0.9%), 18-39y DDTV: 339 (9.2%), 18-39y living donor LT (LDLT): 589 (16.0%), ≥40y DDWG: 12 (0.3%), ≥40y DDTV: 47 (1.3%), and ≥40y LDLT: 133 (3.6%). LDLT groups had lower CIT 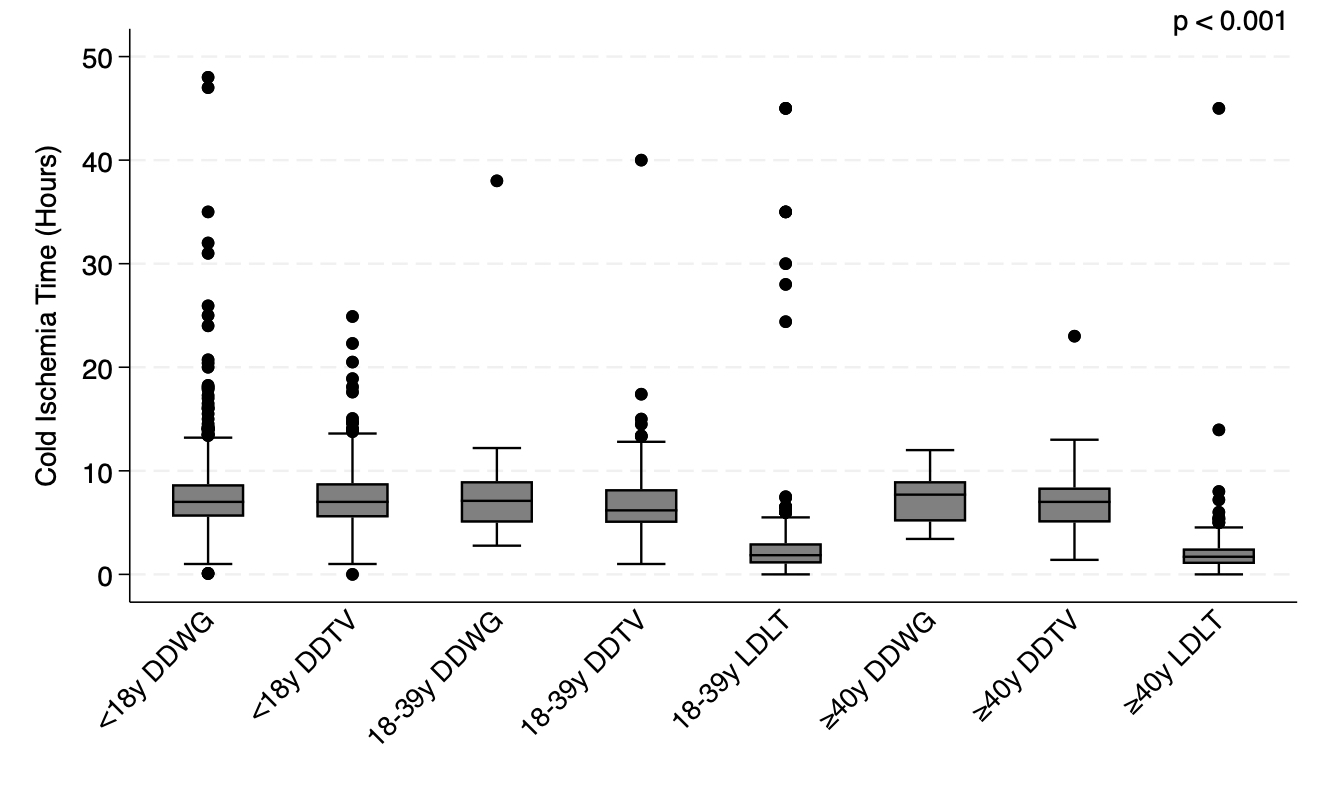 . In multivariable Cox regression, 18-39y LDLT donors were associated with decreased risk of mortality (HR=0.57, 95%CI: 0.32-0.99, p=0.049), while ≥40y DDTV donors (HR=5.13, 95%CI: 2.73-9.65, p<0.001), PVT (HR=1.81, 95%CI: 1.14-2.89, p=0.01), ICU status (HR=1.70, 95%CI: 1.19-2.44, p=0.004), and increasing CIT (HR=1.03, 95%CI: 1.00-1.07, p=0.03) were associated with increased risk of mortality. In multivariable Cox regression, 18-39y LDLT donors (HR=0.51, 95%CI: 0.36-0.73, p<0.001) and recipients ≥2y (HR=0.71, 95%CI: 0.55-0.92, p=0.01) were associated with decreased risk of graft loss, while ≥40y DDTV donors (HR=3.91, 95%CI: 2.52-6.08, p<0.001, PVT (HR=1.41, 95%CI: 1.01-1.96, p=0.0045), and ICU status (HR=1.56, 95%CI: 1.22-1.99, p<0.001) were associated with increased risk of graft loss.
. In multivariable Cox regression, 18-39y LDLT donors were associated with decreased risk of mortality (HR=0.57, 95%CI: 0.32-0.99, p=0.049), while ≥40y DDTV donors (HR=5.13, 95%CI: 2.73-9.65, p<0.001), PVT (HR=1.81, 95%CI: 1.14-2.89, p=0.01), ICU status (HR=1.70, 95%CI: 1.19-2.44, p=0.004), and increasing CIT (HR=1.03, 95%CI: 1.00-1.07, p=0.03) were associated with increased risk of mortality. In multivariable Cox regression, 18-39y LDLT donors (HR=0.51, 95%CI: 0.36-0.73, p<0.001) and recipients ≥2y (HR=0.71, 95%CI: 0.55-0.92, p=0.01) were associated with decreased risk of graft loss, while ≥40y DDTV donors (HR=3.91, 95%CI: 2.52-6.08, p<0.001, PVT (HR=1.41, 95%CI: 1.01-1.96, p=0.0045), and ICU status (HR=1.56, 95%CI: 1.22-1.99, p<0.001) were associated with increased risk of graft loss.
Conclusion: 18-39y LDLT had optimal survival outcomes for children with BA whereas ≥40y DDTV and CIT increased mortality risk. Further studies are needed to identify modifiable factors after procurement that can improve function in ≥40y DDTV grafts and those with prolonged CIT.


Email: info@splitmeeting.org
If you have any questions during the meeting, please go to the registration desk. Our emails will be monitored sporadically.
REGISTRATION DESK OPENING TIMES