
The Future is in Focus: Nurturing Innovation and Collaboration in Pediatric Liver Transplantation
The WebApp is sponsored by: ![]()
Genetic Testing Strategies for Neonatal Cholestasis and Markers associated with Diagnostic Testing in the NICU
Alyshah Lakhani1, Shivam Joshi2, Alexander Weymann1,3, Carol J Potter1,3, Bimal P Chaudhari3,4, A. Jay Freeman1,3.
1 Division of Pediatric Gastroenterology, Hepatology and Nutrition, Nationwide Children’s Hospital, Columbus, OH, United States; 2Center for Biostatistics, Department of Biomedical Informatics, The Ohio State University, Columbus, OH, United States; 3Department of Pediatrics, Nationwide Children’s Hospital, Columbus, OH, United States; 4Division of Genetic and Genomic Medicine, Nationwide Children’s Hospital, Columbus, OH, United States
Introduction: Cholestasis in the Neonatal Intensive Care Unit (NICU) represents a diagnostic challenge due to a broad differential, including prematurity, nutritional factors and genetic causes. Advances in next generation sequencing (NGS) have expanded the ability to identify genetic etiologies; however, studies comparing diagnostic yield and predictors of diagnostic results for cholestasis in the NICU are limited.
Methods: We retrospectively studied patients at a Level IV NICU with cholestasis and hepatology consultation between January 1, 2015 and December 31, 2024. Microarray, NGS panels and exome/genome sequencing (ES/GS) results were reviewed along with clinical characteristics of patients with diagnostic testing. Diagnostic testing was defined as identification of pathogenic variants causative of cholestasis. Categorical variables were compared using Chi-squared or Fisher’s exact test as appropriate. Continuous variables were compared using Wilcoxon rank sum tests.
Results: Diagnostic yield increased by comprehensiveness: microarray 9% (5/55), NGS panels 10% (12/123) and ES/GS 34% (24/71). Seven patients who had non-diagnostic NGS panels had subsequent diagnostic ES/GS (all after 2018). Compared to patients diagnosed by NGS panels, those diagnosed by ES/GS were younger at time of hepatology consult, had higher peak direct bilirubin and were less likely to have sepsis. 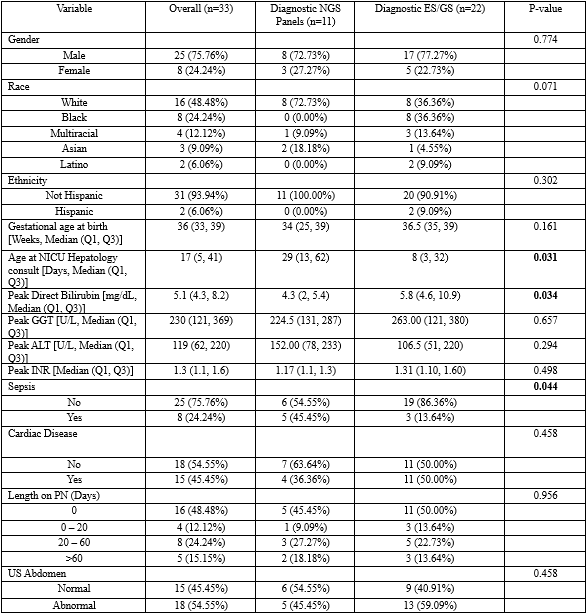
Conclusions: ES/GS demonstrated greater diagnostic yield compared to NGS panels or microarray in cholestatic patients in the NICU. Confounding by year of birth is likely, but the difference in diagnostic yield for ES/GS compared to other forms of testing is large and supports preferential use of ES/GS when a genetic etiology for cholestasis is suspected.


Email: info@splitmeeting.org
If you have any questions during the meeting, please go to the registration desk. Our emails will be monitored sporadically.
REGISTRATION DESK OPENING TIMES