
The Future is in Focus: Nurturing Innovation and Collaboration in Pediatric Liver Transplantation
The WebApp is sponsored by: ![]()
Stability-Selected Machine Learning Identifies Key Determinants of Early Graft Failure in Pediatric Liver Transplantation
Joshua Badshah1, Tyler York1, Megan Adams2, Gregory Tiao1, Thomas Pham1, Stephan Busque1, Marc Melcher1, Varvara Kirchner1.
1Surgery, Stanford University, Stanford, CA, United States; 2Surgery, University of Colorado, Aurora, CO, United States
Introduction
Early graft failure (GF) within 90 days after pediatric liver transplantation remains a major contributor to post transplant morbidity and mortality. Existing risk stratification approaches rely primarily on linear models and limited variable sets, which do not adequately capture the complex and nonlinear relationships between donor factors, recipient illness severity, and early graft outcomes.
Method
Pediatric recipients undergoing first liver transplantation between 2002 and 2025 were identified from a national transplant registry with complete 90 day follow up. Only preoperative donor and recipient variables were included. Data were stratified by outcome and split into training validation and independent test cohorts. Feature selection was performed using L1 regularized regression with repeated subsampling to identify stable predictors. Direction and robustness of selected features were evaluated using L2 coefficients with bootstrap confidence intervals. Multiple machine learning models were trained individually and in ensemble combinations. Model performance was assessed using area under the precision recall curve (AUPR), area under the receiver operating characteristic curve (AUROC), and Brier score.
Results
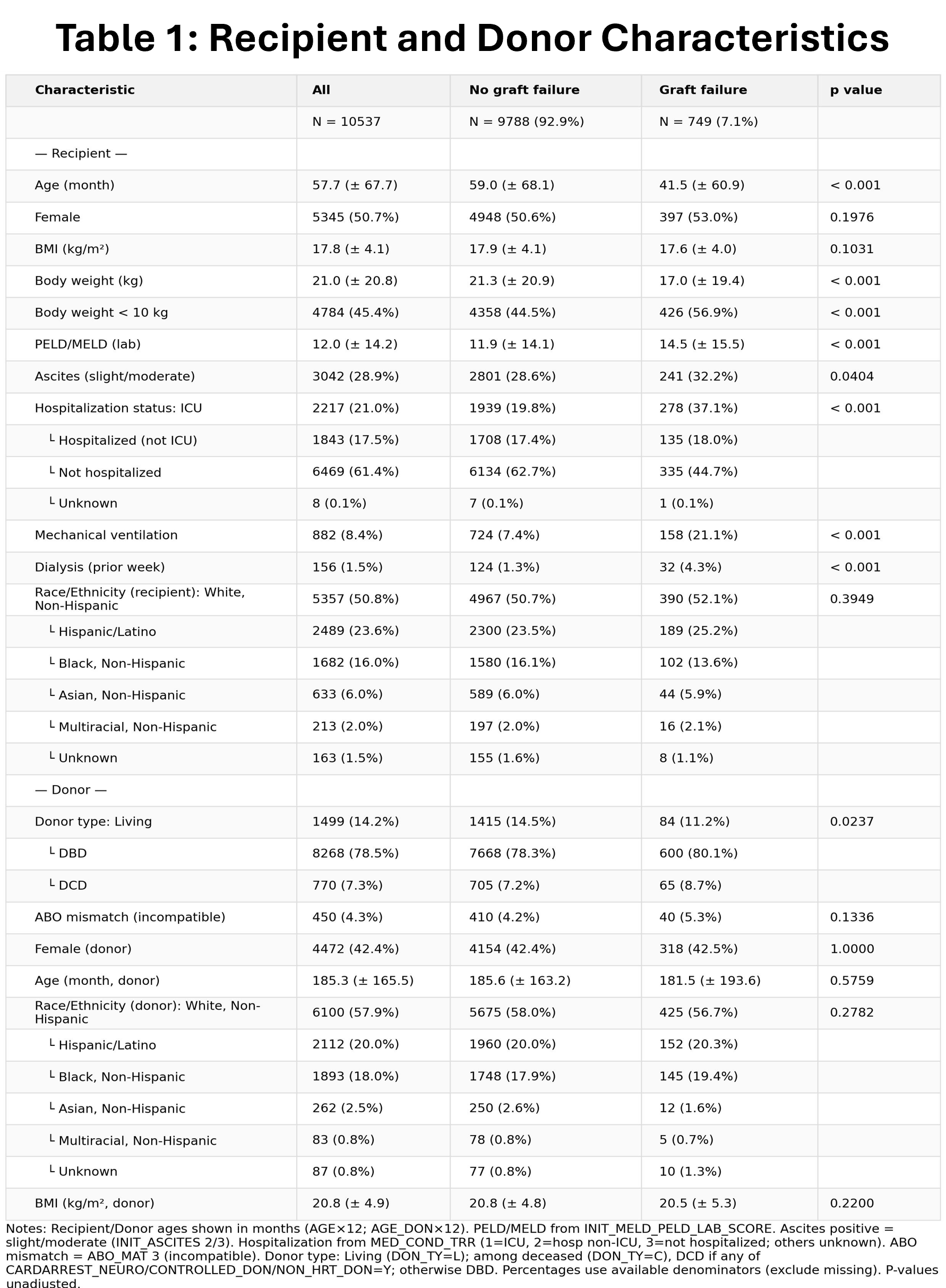
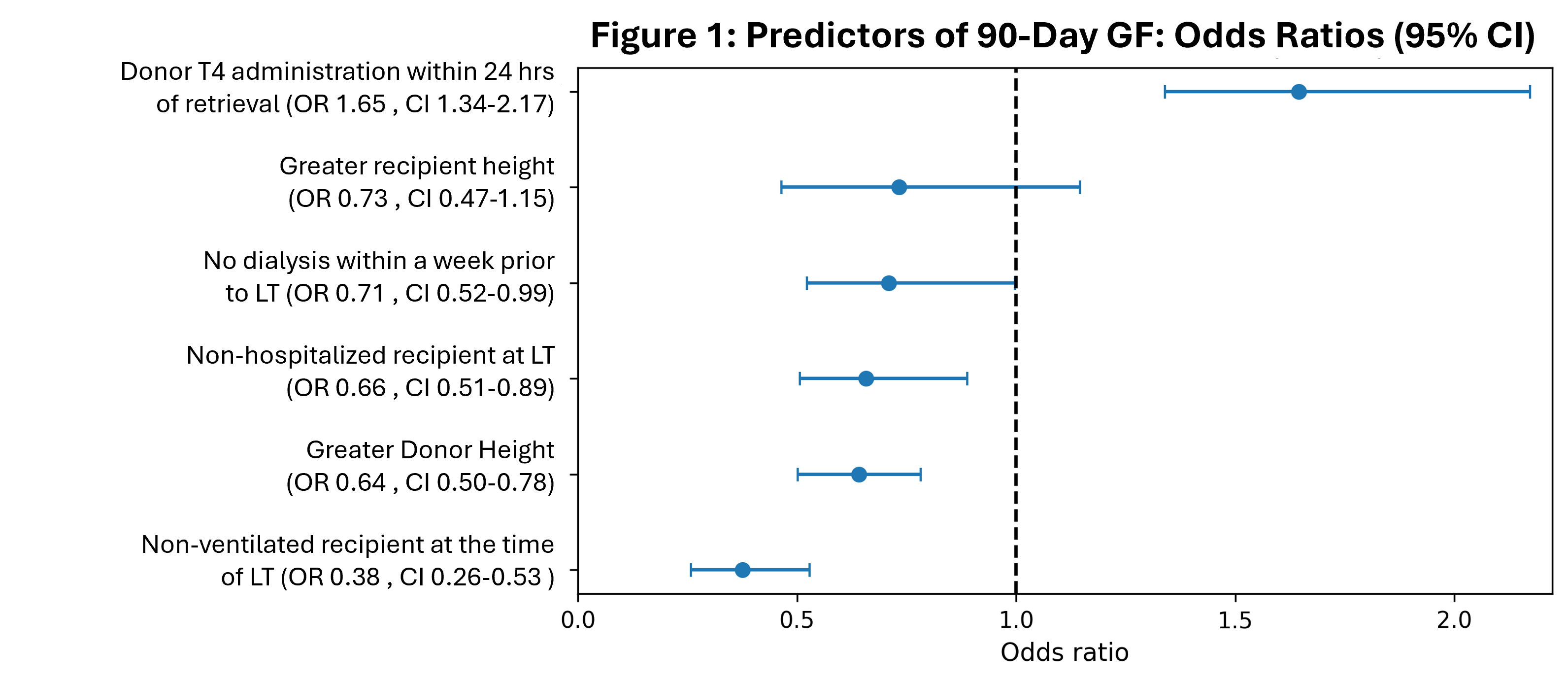
The final cohort included 10,537 pediatric liver transplant recipients, of whom 749 (7.1 percent) experienced graft failure within 90 days. Significant baseline differences were observed between non failure and early graft failure cohorts (Table 1). Stability selection reduced 1,343 transformed features to 53 predictors, six of which demonstrated high stability defined as at least 80 percent selection frequency (Figure 1). Among these six factors, absence of mechanical ventilation at transplant, non-hospitalized status at transplant, absence of dialysis within one week prior to transplant, and greater donor and recipient height were consistently associated with reduced odds of early graft failure. In contrast, donor thyroxine administration within 24 hours of procurement was consistently associated with increased risk of early graft failure.
A mean probability ensemble combining LightGBM and Random Forest achieved the best overall performance, with a test AUPR of 0.156 compared with a baseline prevalence of 0.071, an AUROC of 0.691, and a Brier score of 0.064, demonstrating favorable discrimination and calibration.
Conclusion
Stability guided machine learning identified a small set of clinically interpretable donor and recipient factors associated with early graft failure after pediatric liver transplantation. Ensemble modeling provided modest but clinically meaningful predictive improvement using preoperative data alone, supporting the potential role of stability-based machine learning frameworks in transplant risk stratification and clinical decision support.


Email: info@splitmeeting.org
If you have any questions during the meeting, please go to the registration desk. Our emails will be monitored sporadically.
REGISTRATION DESK OPENING TIMES