
The Future is in Focus: Nurturing Innovation and Collaboration in Pediatric Liver Transplantation
The WebApp is sponsored by: ![]()

Pediatric Surgeon. Pediatric Transplant Surgeon involved in Liver and Intestinal Transplantation, PhD. Also involved in the Intestinal Rehabilitation Field. Pediatric Surgery Residency from 2002-2007 at Hospital La Paz (Madrid, Spain). Visitor fellow in Omaha (nebraska) in 2007-2008. Pediatric Transplant Surgeon from 2009 to 2025. Member of several Transplant Assocations (IRTA; IPTA, SETH; SET; ESOT...). Part of several ERNs (TrasnplantChild, ERNICA). Associated Teacher at University Autonoma of Madrid from 2010.
Auxiliary split-hope liver transplantation from a donation after circulatory death donor as treatment for pediatric acute liver failure: case report
Ane Andres1,2,3, Maria Victoria Lopez-Canelada1, Javier Serradilla1,2,3, Maria Velayos1,2,3, Alba Sanchez-Galan1,3, Alba Bueno4, Wayel Hassem5, Maria Dolores Lledin2,3,6, Luis Seas1, Esteban Frauca2,3,6, Francisco Hernandez-Oliveros1,2,3.
1Pediatric Surgery, La Paz University Hospital, MADRID, Spain; 2La Paz Research Institute, La Paz University Hospital, MADRID, Spain; 3TransplantChild, La Paz University Hospital, MADRID, Spain; 4Transplant Surgery, Birmingham´s Children Hospital, Birmingham, United Kingdom; 5Transplant Surgery, King´s College Hospital, London, United Kingdom; 6Pediatric Hepatology, La Paz University Hospital, MADRID, Spain
Introduction: Acute liver failure (ALF) is associated with significant mortality in pediatric patients. Auxiliary partial orthotopic liver transplantation (APOLT) represents a therapeutic alternative in selected patients with ALF who retain the potential for native liver regeneration.
Case Report: A four-year-old boy presented with ALF secondary to paracetamol intoxication (166 mg/kg/day for 72 hours). At admission, he showed metabolic acidosis (pH 7.07), hyperammonemia (239 µmol/L), severe hypertransaminasemia (AST 14,320 IU/L; ALT 4,992 IU/L), coagulopathy (INR 3.8), grade III/IV hepatic encephalopathy, and acute kidney injury (creatinine 0.81 mg/dL), with rapid deterioration despite standard conservative management.
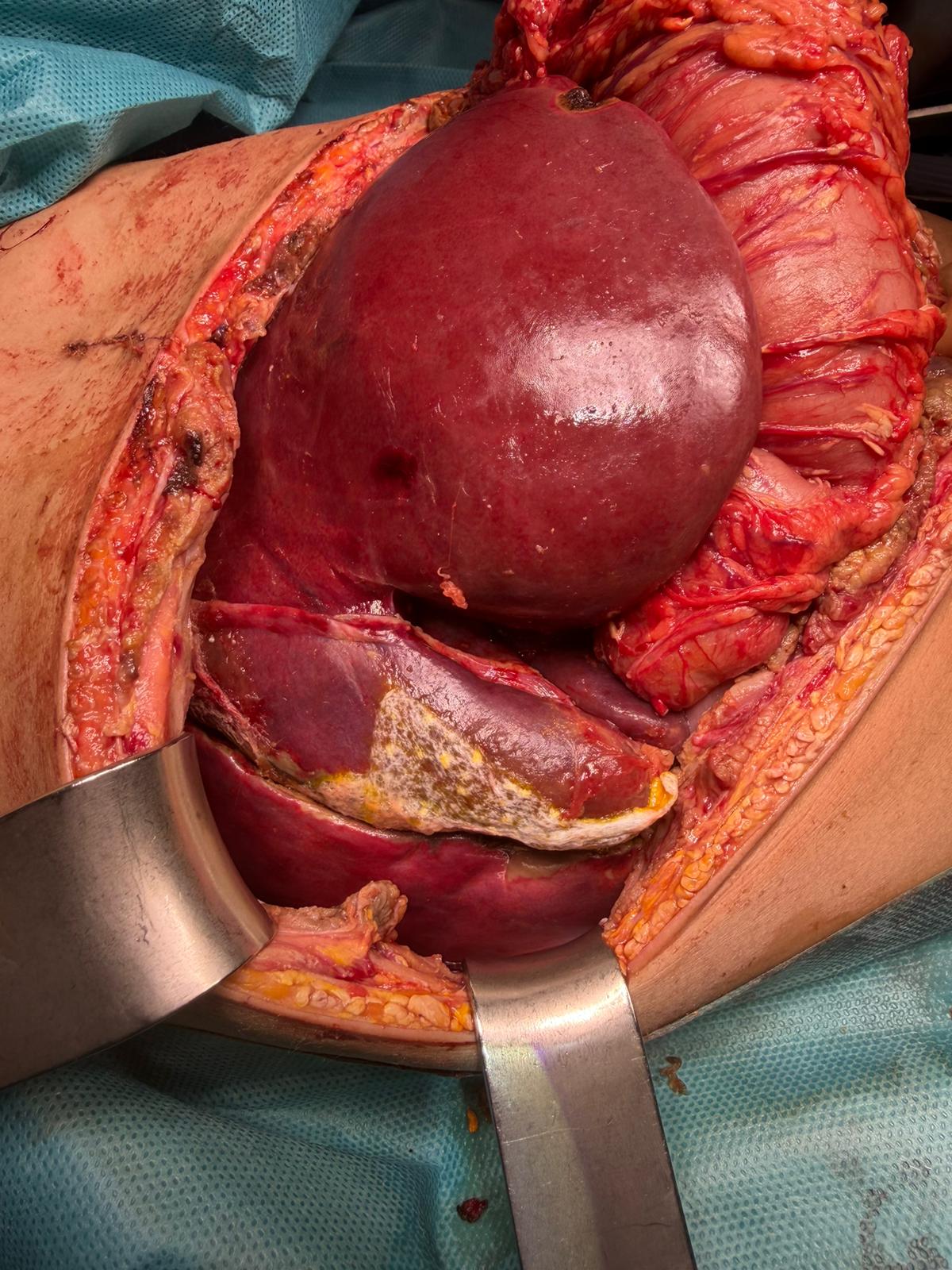
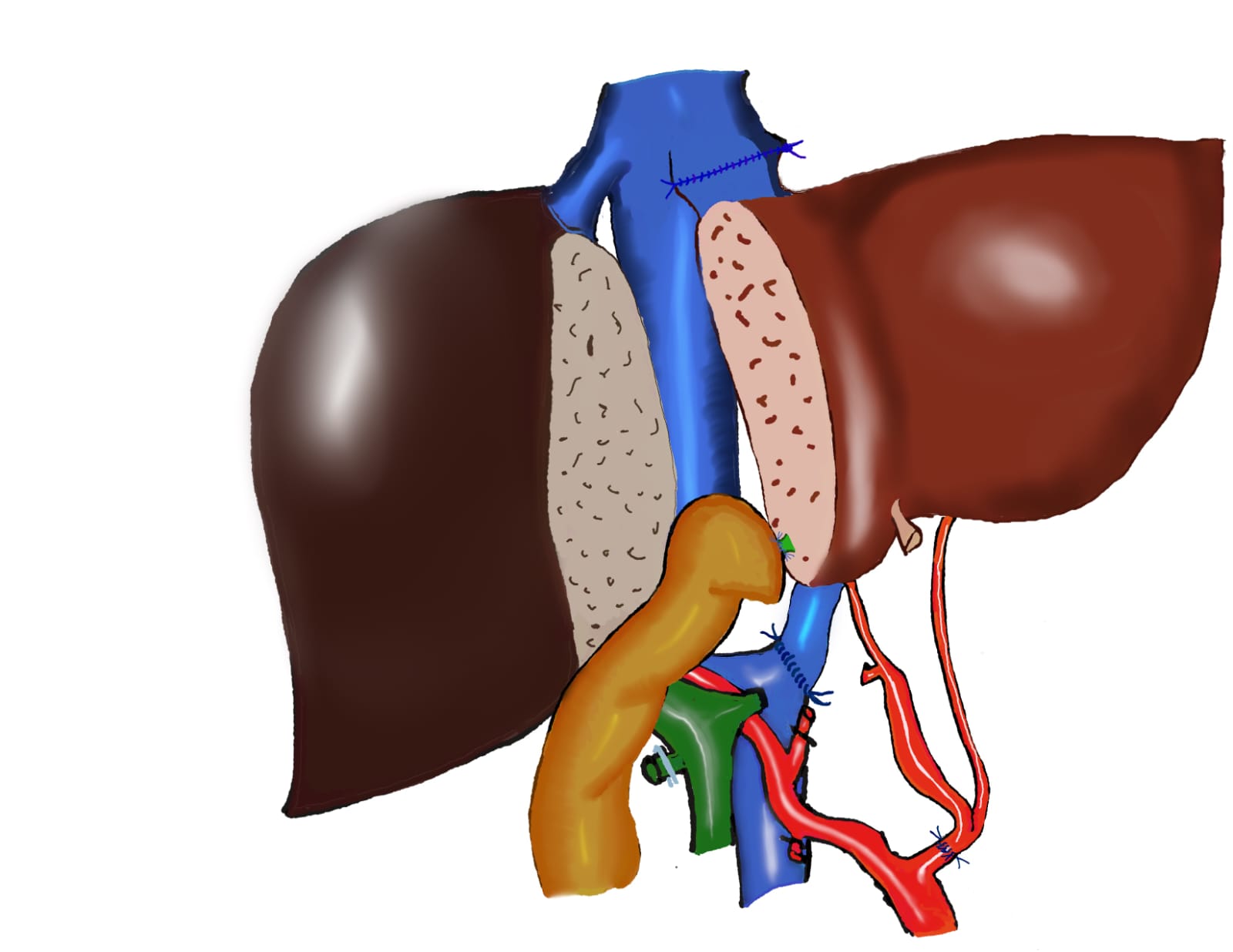
APOLT was performed 48 hours after admission using a donation after circulatory death (DCD) donor. An ex-situ liver split was carried out under hypothermic oxygenated perfusion (HOPE), implanting segments II–III–IV (graft-to-recipient weight ratio 1.78%). The right liver graft was successfully transplanted into an adult recipient. An extended left hepatectomy was performed, preserving segments VI–VII, along with a temporary portocaval shunt. The graft was implanted orthotopically with portal-to-portal anastomosis, recipient left hepatic vein anastomosed to the graft middle and left hepatic veins, common hepatic artery to recipient splenic artery, and Roux-en-Y biliary reconstruction.
Postoperative complications included a biliary leak requiring surgical repair and acute pancreatitis related to ALF. One month after transplantation, the patient showed normal hepatic, renal, and neurological function, with 65% recovery of native liver parenchyma. Progressive immunosuppression withdrawal and auxiliary graft removal are planned.
Conclusion: DCD donation with normothermic regional perfusion followed by split-HOPE represents an alternative organ source that enables auxiliary liver transplantation in critically ill pediatric patients with acute liver failure.


Email: info@splitmeeting.org
If you have any questions during the meeting, please go to the registration desk. Our emails will be monitored sporadically.
REGISTRATION DESK OPENING TIMES