
The Future is in Focus: Nurturing Innovation and Collaboration in Pediatric Liver Transplantation
The WebApp is sponsored by: ![]()
Selection, Timing, and Outcomes of Pediatric Liver Transplantation for Malignant Liver Tumors
Simone Santoro Angelo Zaragoza1, Haaris Kadri2, Tobias S Broering 3, Joseph Tector III4, Richard Mangus1, Phillipe Abreu5.
1Department of Surgery, Indiana University School of Medicine, Indianapolis, IN, United States; 2Anschutz Medical Campus, University of Colorado School of Medicine, Aurora, CO, United States; 3Department of General, Visceral and Thoracic Surgery, University Medical Center Hamburg-Eppendorf, Hamburg, Germany; 4Miami Transplant Institute, Jackson Memorial Hospital - Hospital of Miami, Miami, FL, United States; 5Department of Surgery, University of Colorado School of Medicine, Aurora, CO, United States
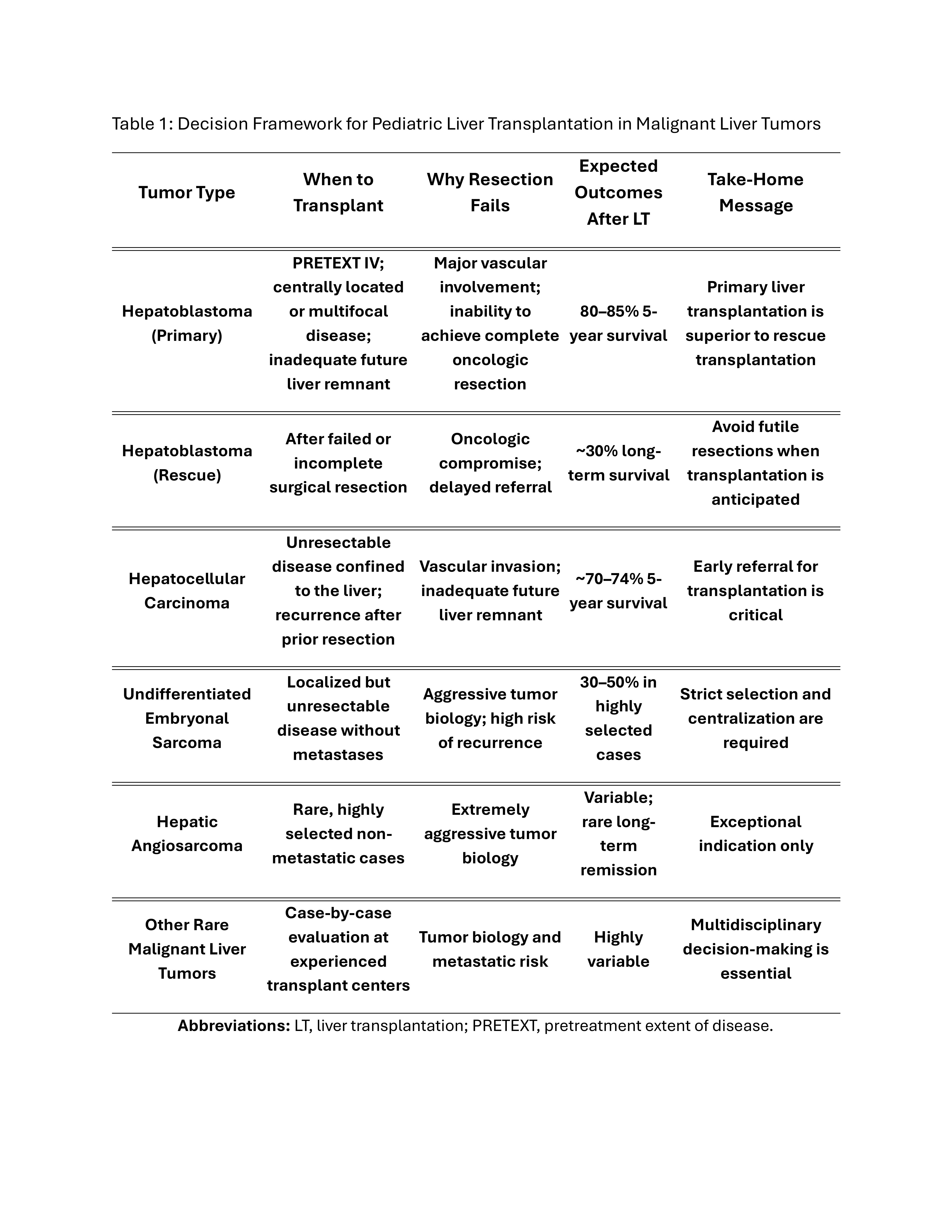
Introduction: Pediatric malignant liver tumors represent a rare but high-risk indication for liver transplantation (LT). In this population, outcomes are highly dependent on appropriate patient selection and timing of transplantation, particularly when balancing primary transplantation versus attempted resection and rescue transplantation.
Method: A structured literature review was performed to evaluate outcomes of pediatric LT for hepatoblastoma (HB), hepatocellular carcinoma (HCC), and rare malignant liver tumors. Emphasis was placed on transplant-specific decision factors, including resectability, timing of listing, recurrence, and survival.
Results: Approximately 10–20% of children with HB ultimately require LT. Primary LT is consistently associated with superior outcomes, with reported 5-year survival rates of 80–85%, compared with markedly inferior survival following rescue transplantation after attempted resection. In pediatric HCC, LT offers potential cure when the disease is confined to the liver but remains limited by post-transplant recurrence, resulting in a 5-year survival of approximately 70%. For rare malignant liver tumors, including undifferentiated embryonal sarcoma and hepatic angiosarcoma, LT can achieve meaningful survival (30–50%) in highly selected patients when performed at experienced, high-volume centers.
Conclusion: Outcomes after pediatric liver transplantation for malignant tumors are driven primarily by appropriate candidate selection and listing timing. Early recognition of unresectability, avoidance of futile resections, and referral to specialized transplant centers represent the most modifiable factors to improve survival and optimize graft utilization in pediatric transplant oncology.


Email: info@splitmeeting.org
If you have any questions during the meeting, please go to the registration desk. Our emails will be monitored sporadically.
REGISTRATION DESK OPENING TIMES